

Abstract
Glucocorticoids are potent anti-inflammatory drugs used for a variety of chronic diseases and acute conditions that, unfortunately, can also cause severe adverse events. Venous thromboembolism (VTE) has recently been added to the list of clinical complications associated with glucocorticoids. Epidemiological studies reported that the risk for first VTE is increased by 2 to 3-fold with the use of glucocorticoids. However, several confounders may account for the reported association and whether glucocorticoid use increases the risk of recurrent VTE is unknown. To address the issue of confounding, we determined the frequency of a first VTE event associated with the use of oral glucocorticoids employing the self-controlled case-series (SCCS) method. With SCCS every individual is contrasted with him or herself thereby eliminating fixed confounders such as age, sex or chronic comorbidity. In addition, we evaluated the effect of oral glucocorticoids on the risk of recurrent VTE in a cohort design.
Patients with VTE from the MEGA study were individually linked to the Dutch Foundation for Pharmaceutical Statistics (SFK). Prescriptions of oral glucocorticoids in the period of the MEGA study were identified. The risk for the first VTE was estimated using SCCS method and conditional Poisson regression. The association between oral glucocorticoids and recurrent VTE was examined using age and sex adjusted Cox regression models.
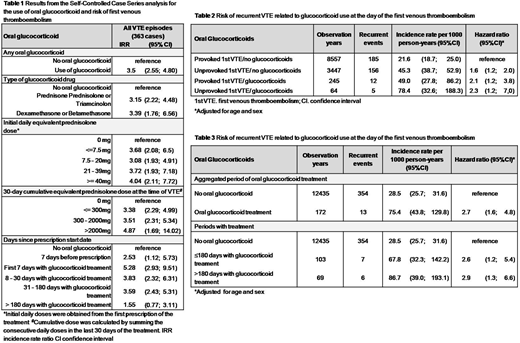
A total of 2547 patients could be linked to the SFK data register, from those 363 received at least one outpatient prescription of oral glucocorticoids. The risk for a first VTE event was 3.5-fold higher in the aggregated period of oral glucocorticoid treatment as compared with baseline periods (incident rate ratio [IRR] 3.5, 95% confidence interval [CI] 2.6-4.8). IRR of a first VTE event was 2.5 (95% CI, 1.1- 5.7) in the week before treatment started, 5.3 (95% CI, 2.9 - 9.5) during the first 7 days with treatment, 3.7 (95% CI, 2.6 - 5.2) until six months with treatment and 1.6 (95% CI, 0.8 - 3.1) after 6 months with oral glucocorticoids, as compared with the baseline period. A dose-dependent relationship between oral glucocorticoid treatment and VTE risk was observed as the IRR increased from 3.4 (95% CI, 2.3 - 5.0) with 30-day cumulative doses below 300mg to 4.9 (95% CI, 1.7 - 14.0) with 30-day cumulative doses above 2000mg, as compared with baseline periods. IRRs for DVT (3.9; 95% CI, 2.9 - 9.5) and PE (3.1; 95% CI, 2.0 - 4.9) were similar and IRR for unprovoked VTE (2.4; 95% CI, 1.3 - 4.7) was lower than the IRR for provoked VTE (4.2; 95% CI, 2.9 - 6.0). The rates of recurrent VTE were elevated in patients with unprovoked VTE and in those who had their first VTE during a period of oral glucocorticoid treatment, either if the first event was otherwise classified as provoked or unprovoked. The adjusted HR for recurrent VTE was 1.6 (95% CI, 1.2 - 2.0) in patients with unprovoked first VTE not using oral glucocorticoids at the time of their first event, 2.1 (95% CI, 1.2 - 3.8) in those who had a provoked first VTE while using oral glucocorticoids and 2.3 (95% CI, 1.2 - 7.0) in those with an unprovoked first VTE while using the drug, as compared with patients with a provoked first event not using oral glucocorticoids at the time of their first event. The risk for recurrent VTE was 2.7-fold increased (95% CI, 1.6 - 4.8) during glucocorticoid treatment periods as compared to baseline periods.
We conclude that patients receiving oral glucocorticoids had an approximately three-fold increase in the risk for first and recurrent VTE. The observed risk for VTE was partly associated with the underlying disease (preexposure period) and increased further after oral glucocorticoids were prescribed. These results underscore that treatment strategies to prevent first and recurrent VTE in patients treated with oral glucocorticoids are needed.
No relevant conflicts of interest to declare.

